
In the case of AT, various entities can be clearly distinguished from one another, since these sometimes differ significantly in both pathogenesis and therapy:
- Midportion tendinopathy (MPT): typical thickening, usually pressure-dolent, in the middle third of the tendon, usually between 3 – 5 (–7) cm proximal to the insertion.
- Insertional tendinopathy (IT): between 0–3 cm proximal to the insertion. Often associated with Haglund exostosis.
- Insertional intratendinous calcifications (IV): deep distal at the calcaneal insertion, often asymptomatic.
- Special forms include, for example, medication-associated tendinopathies. These are usually caused by treatment with corticoids or the use of fluoroquinolone antibiotics.
Causes
While biomechanical and functional causes must always be sought to explain the pathogenesis of MPT, IT is often additionally caused by a primary mechanical factor in the presence of Haglund exostosis. This leads to impingement with the Achilles tendon in dorsiflexion in the ankle and can lead to circumscribed ventral partial lesions at the calcaneal insertion.
In addition, runners must be careful to wear running shoes that fit their feet / foot position to avoid tilting in the hindfoot, which can lead to shear forces on the Achilles tendon. Tendonopathies also occur more frequently in patients with diabetes, renal insufficiency, obesity or high uric acid levels. Likewise, the use of corticosteroids, statins and fluoroquinolone antibiotics (FQ) should be enquired about, as these can lead to spontaneous ruptures of the Achilles tendon [4].
Diagnostics
- Clinical examination / functional testing
- Sonography incl. colour Doppler
- MRI
- X-ray calcaneus lateral
- Treadmill analysis / foot pressure measurement
- Electromyography (EMG)
- Elastrography
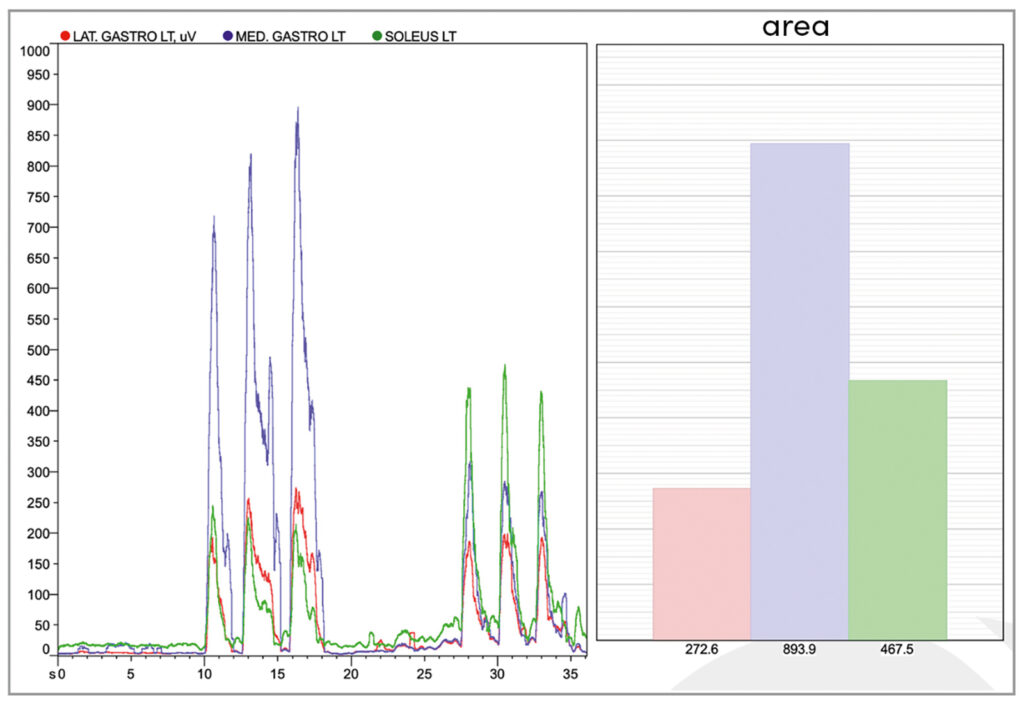
In recent years, EMG has become increasingly important as it offers the possibility of identifying control disorders of the musculature (Fig. 1), developing EMG-controlled individualised exercises for patients and, in difficult cases, conducting biofeedback training.
Therapy
At the beginning of therapy, the severity of the clinical symptoms and the results of the imaging determine whether athletes can initially be left with a reduction in training volume or a reduction in the load on the Achilles tendon, or whether a break from sport is necessary. The basic therapy in all cases is the elimination of biomechanical risk factors and incorrect loading by means of functional training. Existing foot misalignments / tilting of the hindfoot should be compensated for with insoles if necessary. Manual mobilisation of the foot and ankle plays an important role alongside the classic therapeutic procedures on the tendon itself. Care should be taken to ensure that the ankle is as mobile as possible. For example, a 3.5-fold increase in the likelihood of developing Achilles tendon tendinopathy has been observed in patients with ankle dorsiflexion of less than 11.5° [5]. Other risk factors include reduced plantar flexion strength and hypomobility in the talonavicular joint. The knee-to-wall test is a simple and valid tool for an orienting examination.
Nutrition
From a nutritional point of view, it is recommended to reduce or avoid purine-rich / uric acid-increasing foods (especially meat and offal). An adequate intake of omega-3 fatty acids is important. The anthocyanin contained in cherries (mainly Montmorency sour cherries) has an anti-inflammatory effect, reduces oxidative stress and lowers uric acid levels. The celabin A contained in curcumin upregulates the transcription factor scleraxis [6]. This in turn promotes the proliferation of tenocytes and thus collagen I synthesis and the formation of the extracellular matrix. Incense (Boswellia), which is often found in food supplements together with curcumin, has a similar effect. Bromelain stimulates, among other things, the formation of new tenocytes.
Eccentric training (ET)
A well-known and effective form of training is ET with 3 x 15 repetitions twice a day over a period of 8 – 12 weeks. It should be ensured that the exercises are performed with both the knee extended (M. gastrocnemius) and with the knee bent (M. soleus). If IT is present, these exercises should only be performed up to the neutral position of the ankle to avoid impingement of the Haglund’s deformity, which is usually present. Good results were then seen in 67 % of cases, while improvement only occurred in 28 %–32% when training was extended into dorsiflexion [7]. However, current data show that PTLEs (Progressive Tendon Loading Exercises) are sometimes more effective than pure ET and can therefore be recommended as initial conservative therapy [8]. Although Cook and Rio’s 4-stage progressive loading protocol [9] was originally developed for tendinopathy of the patellar tendon, it can also be used to treat AT when adapted to the Achilles tendon.
Extracorporeal shock wave therapy (ESWT)
ESWT is now used almost universally in the treatment of Achilles tendinopathy. Korakasis et al. [10] were able to show that the effect of conservative therapy in combination with ESWT is better in the short, medium and long term than without it. Other studies also show that ESWT alone, without adequate basic therapy, is of no benefit. Both radial and focused shock waves have been shown to produce good results on the tendon itself. However, it has also been shown that ESWT does not lead to any improvement in symptoms in IT compared to eccentric training alone [1, 11].
Infiltration
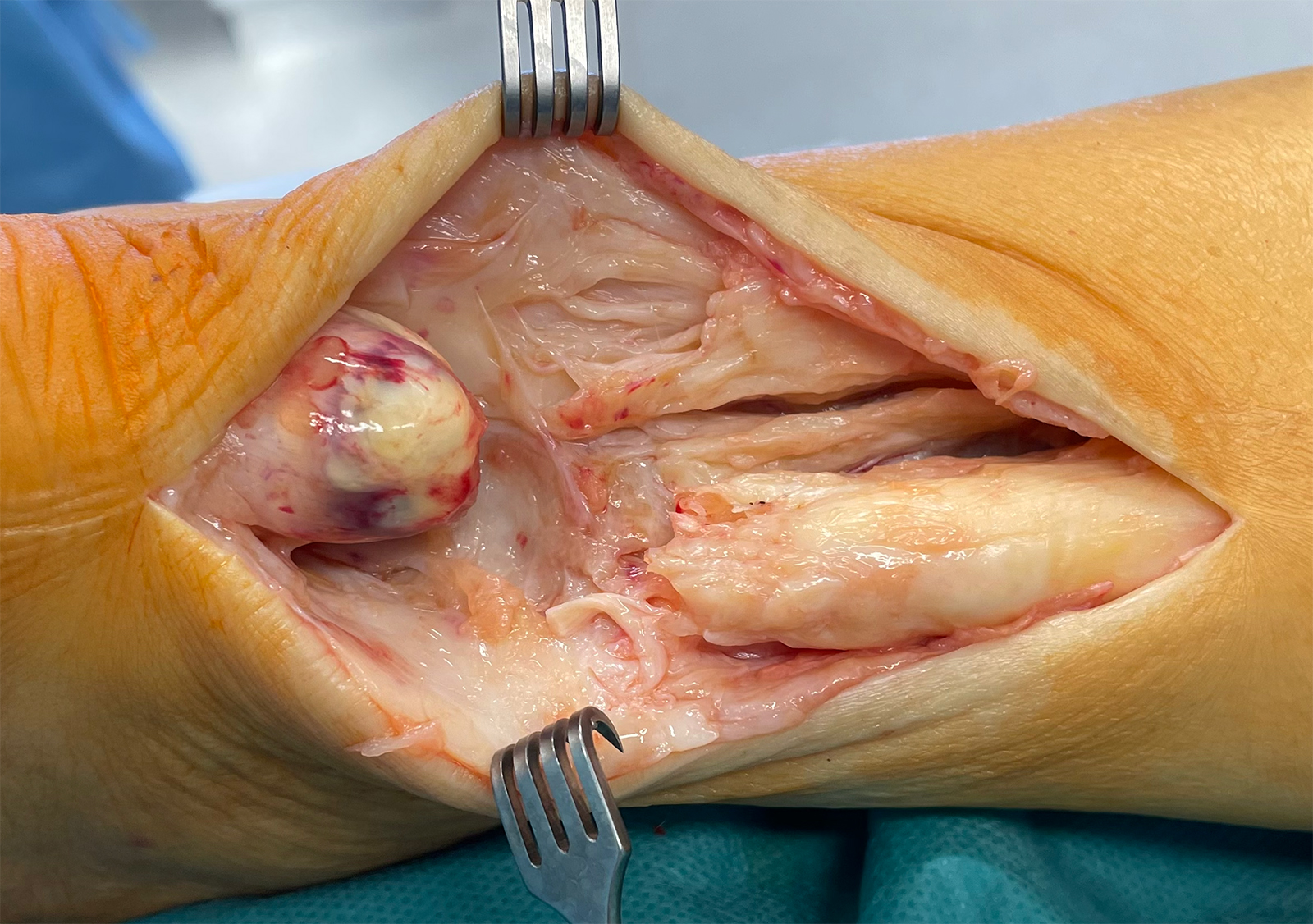
Infiltration of the Achilles tendon with hyaluronic acid (HA), PRP or substances such as Traumeel®, embedded in a differentiated treatment concept, show good results. For example, for peritendinous infiltration of the Achilles tendon with hyaluronic acid, a reduction in pain and tendon thickness as well as a decrease in neovascularisation could be shown in both MPT and IT [12]. We recommend that the infiltrations be performed under ultrasound guidance in order to safely reach the peritendinous space. In addition, infiltrations can be performed almost painlessly. Sclerotherapy is a special form of treatment used to close sprouting neo-vessels. In cases of severe neovascularisation, it can quickly reduce pain. Infiltrations must be strictly extra-tendinous, ultrasound-guided and should only be performed by experienced therapists. Infiltrations in the tendon and bursa area with any type of corticosteroid should be avoided at all costs due to the potential for devastating tendon damage (Fig. 2).
USGET, EPI
In ultrasound-guided galvanic electro-physis therapy (USGET, EPI), acupuncture needles are placed under ultrasound guidance in the tendinopathy and microcurrents are applied via these (Fig. 3). This therapy stimulates the tenocytes to produce collagen. Depending on the pain experienced during treatment, the tendon can be infiltrated with a local anaesthetic under ultrasound guidance immediately beforehand in order to achieve sufficiently high currents. This has been shown to result in faster healing than with physiotherapy alone, although further studies with larger case numbers are certainly needed [13].

b visualisation of the acupuncture needle during electrolysis; c therapeutic setting © Firma Gymna
Surgical procedures
If conservative treatment fails, established surgical procedures are available for treating both MPT and IT. These include tenolysis of the tendon itself, with removal of the diseased tendon parts, and, in the case of IT, of the Haglund exostosis and possible intratendinous calcifications. In recent years, the influence of the plantar fascia tendon, which often runs medially to the Achilles tendon, has come into focus. In the case of MPT manifested in the medial buttress and sometimes visible annular ligament or existing adhesions, this must be addressed [14, 15].
Conclusion
The treatment of Achilles tendon tendinopathy is complex. Differentiated clinical and imaging diagnostics are required to make an accurate diagnosis. A distinction must be made between mid-portion and insertion tendinopathy, both in terms of pathogenesis and therapy. In recent years, dietary supplements such as curcuma, boswellia and others, as well as new therapeutic methods such as ultrasound-guided electrolysis therapy, have been established alongside classic methods. Surgical procedures are available in the event of failure of conservative therapy. Here, the focus has shifted to MPT caused by adhesions of the plantar fascia tendon.
Bibliography
[1] Paantjens, MA, Helmhout PH, Backx F, Martens M, van Dongen J, Bakker E: Intra- and Inter-Rater Reliability of Processing Ultrasound Tissue Characterization Scans in Midportion Achilles Tendinopathy. Transl Sports Med 2022 Jun 16: 2022: 9348298
[2] Mifsud, T, Gatt A, Micallef-Stafrace K, Chocklingam N, Padhiar N: Elastography in the assessment of the Achilles tendon: a systematic review of measurement properties. J Foot Ankle Res. 2023 Apr 27; 16(1):23
[3] Gatz M, Betsch M, Dirrichs T, Schrading S, Tingart M, Michalik R, Quack V: Eccentric and Isometrich Exercises in Achilles Tendinopathy Evaluated by the VISA-A Score and Shear Wave Elastography. Sports Health. 2020 Jul/ Aug; 12(4): 373-381
[4] Tsai WC, Yang YM: Fluoroquinolone-associated Tendinopathy. Gung Med J. 2011 Sep-Oct; 34(5): 461-7
[5] Jayaseelan DJ, Kecman M, Alcorn D, Sault JD: Manual therapy and eccentric in the management of Achilles tendinopathy. J Man Manip Ther. 2017 May; 25(2): 106-114
[6] Gumucio J, Schonk M, Kharaz Y, Comerford E, Mendias C: Scleraxis is required for the groth of adult tendons in response to mechanical loading. JCI Insight. 2020 Jul 9; 5(13)
[7] Dilger C, Chimenti R: Nonsurgical Treatment Options for Insertional Achilles Tendinopathy. Foot Ankle Clin 2019 Sep; 24(3): 505-513
[8] Breda S, Oei E, Zwerver J, Visser E, Waarsing E, Krestin G, de Vos RJ: Effectiveness of progressive tendon-loading exercise therapy in patients withpatellar tendinopathy: a randomized clinical trial. Br J Sports Med. 2021 May; 55(9): 501-509
[9] Milliards P, Cook J, Purdam C, Rio E: Patellar Tendinopathy: Clinical Diagnosis, Load Management and Advice for Challenging Case Presentatations. J Orthop Sports Phys Ther 2015; 45(11): 887-98
[10] Korakakis V, Whiteley R, Tzavara A, Malliaropoulos N: The effectiveness of extracorporeal shockwave therapy in common lower limb conditions: a systematic review including quantification of patient-rated pain reduction. Br J Sports Med 2018 Mar; 52(6): 387-407
[11] Mansur N, Matsunaga F, Carrazzone O, dos Santos B, Nunes C, Aoyama B, dos Santos P, Faloppa F, Tamaoki M: Shockwave Therapy Plus Eccentric Exercises Versus Isolated Eccentric Exercises for Achilles Insertional Tendinopathy: A Double-Blinded Randomized Clinical Trial. J Bone Joint Surg Am. 2021 Jul 21; 103(14): 1295-1302
[12] Folgi M, Giordan N, Mazzoni G: Efficacy and safety of hyaluronic acid (500-730 kDa) Ultrasound-guided injections on painful tendinopathies: a prospective, open label, clinical study. Muscles Ligaments Tendons J 2017. 2017 Sep 18; 7(2): 388-395
[13] Asensio-Olea L, Leiros R, Marquez-Sanchez M, Oliviera de Carvalho F, Maciel L: Efficacy of percutaneous electrolysis for the treatment of tendinopathies: A systematic review and meta-analysis. Clin Rehabil. 2023 Jun; 37(6): 747-759
[14] Alfredson H, Masci L, Spang C: Ultrasound and surgical inspection of plantaris tendon involvement in chronic painful insertional Achilles tendinopathy: a case series. BMJ Open Sport Exerc Med. 2021 Mar 22; 7(1)
[15] Masci L, Neal B, Bee W, Spang C, Alfredson H: Achilles Scraping and Plantaris Tendon Removal Improves Pain and Tendon Structure in Patients with Mid-Portion Achilles Tendinopathy-A 24 Month Follow-Up Case Serie. J Clin Med. 2021 Jun 18; 10(12): 2695
Autoren

ist Facharzt für Orthopädie und Unfallchirurgie mit Zusatzbezeichnungen Sportmedizin und Notfallmedizin. Er ist Inhaber der Praxis SPORTORTHO rheinmain in Bad Homburg und war langjähriger Mannschaftsarzt u. a. in der Fußball-Bundesliga (Eintracht Frankfurt, TSG 1899 Hoffenheim) und ist Kooperationsarzt verschiedener Vereine und Athleten insbesondere in den Bereichen Fußball, Leichtathletik, Handball, Bob.

ist Fachärztin für Orthopädie und Unfallchirurgie mit Zusatzbezeichnungen Akupunktur und Notfallmedizin. Sie ist in der SPORTORTHO rheinmain in Bad Homburg tätig und betreut Sportler verschiedener Disziplinen (Schwerpunkt Leichtathletik).

hat einen Masterabschluss im Bereich Sportphysiotherapie an der DSHS Köln gemacht. Sie leitet in der SPORTORTHO rheinmain in Bad Homburg den Bereich EMG und funktionelle Diagnostik. Dort behandelt und betreut sie Sportler insbesondere aus den Bereichen Leichtathletik, Fußball und Handball.


