
According to the BMA guide to sport injuries [1], shoulder injuries in water sport athletes rank in the top five most common injuries. These include shoulder joint injuries with and without dislocation, rotator cuff injuries, disorders of the tendons (tendinitis) and arthritis.
These clinical pictures may have or may acquire degenerative and inflammatory components. To avoid the indicated surgery, where applicable, but also as follow-up treatment after surgery, another treatment that can be used alongside and supplementary to the generally accepted indicated treatments is infiltration with various substances. Corticoids were and are popularly used for injection treatments. Both the corticoids and local anaesthetics are effective in treating acute pain but are also reputed to be potentially cytotoxic and to hinder healing. On the other hand, the supply of oxygen and nutrients to damaged structures and their metabolic and structural integrity must be rapidly restored. Are there any (biological) alternatives?
Blood cell secretome (BCS)
BCS (Orthokine) is a cell-free cocktail of all the factors quantitively released from the blood cells during coagulation. These factors initiate regeneration/wound healing after wound closure. They are released under controlled conditions at 37 oC using the medical device EOT II. Although the healing effect cannot be attributed to one single factor alone, the role of the various growth factors in BCS in tissue healing has been established (e.g. TGF, HGF, IGF, PDGF, FGF). Other BCS components to which an effect can be attributed are cytokines, lipid mediators and extracellular vesicles.
Case study shoulder injury

Fig. 1 Before treatment: MRI of the affected left shoulder. Clearly visible bursitis and joint effusion as well as damage to the supraspinatus tendon.
A female water polo player (29) presented at our practice with pain and loss of strength in her left shoulder. She usually trained 6 times a week and had already struggled painfully through her last matches. Clinically, ultrasound showed well marked subacromial bursitis, which was apparently not caused by trauma, and a partial supraspinatus tendon tear in the left shoulder (see also Fig.1). She received conservative treatment with targeted physiotherapy and osteopathy to improve/optimise function/biomechanics over a period of two months with concomitant gentle loading and cooling treatment. Puncture of the subacromial bursa and 1x subacromial bursa infiltration with corticoids were also performed.
Four weeks after the corticoid infiltration, BCS was infiltrated four times on the supraspinatus tendon under ultrasound control (every 3 – 4 days, 2 mL per infiltration). After the first infiltration, the patient already reported reduced pain, after the third, freedom from pain at rest, and after the fourth, only minimal pain under loading. Additional concomitant measures included function analysis, function training and dry needling. Ultrasound follow-up after three months showed marked structural improvement in the supraspinatus tendon. The patient continues to report freedom from pain under full loading. We attach ultrasound images for information purposes (Figs. 2 and 3), being well aware that ultrasound images are not comparable to ”initial MRI images“.
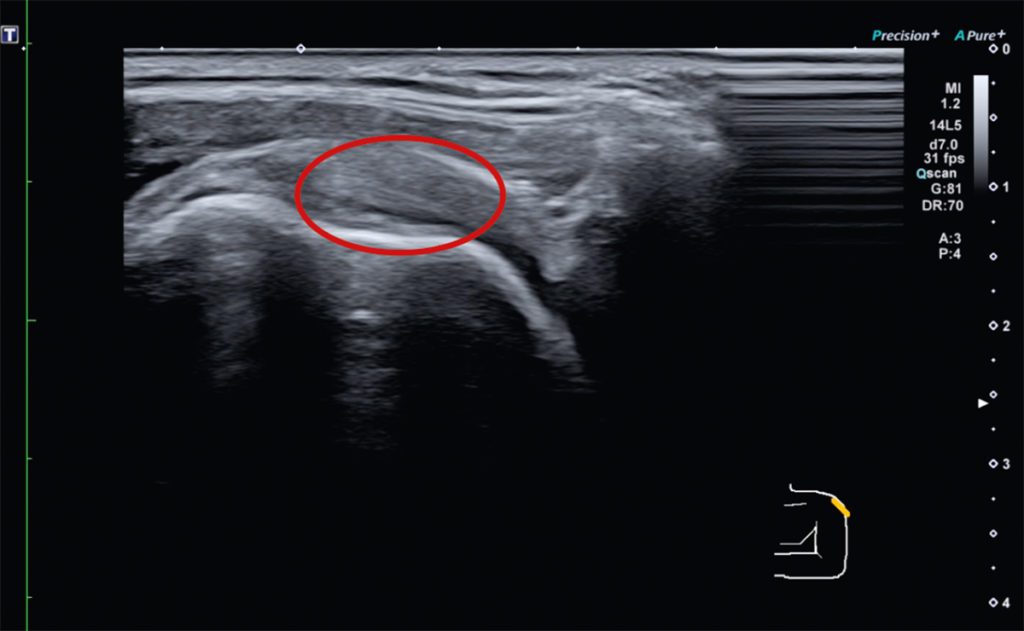 Fig. 2 Before treatment: ultrasound image of the affected left shoulder. Visible supraspinatus tendon tear.
Fig. 2 Before treatment: ultrasound image of the affected left shoulder. Visible supraspinatus tendon tear.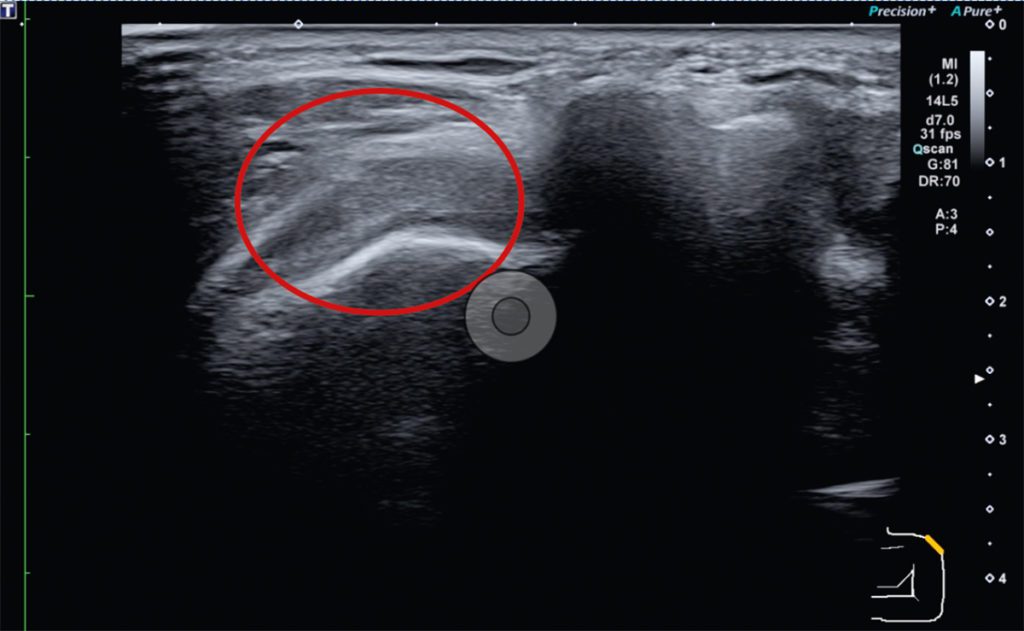 Fig. 3 Follow-up after 3 months: ultrasound image of the affected left shoulder. Visible structural improvement in the supraspinatus tendon tear.
Fig. 3 Follow-up after 3 months: ultrasound image of the affected left shoulder. Visible structural improvement in the supraspinatus tendon tear.Currently available studies on BCS
A study on supraspinatus tendinopathy published in 2018 shows that infiltration with BCS is markedly superior to a corticoid in the medium term [2]. A series of earlier studies show improved healing of tendons and muscles with BCS in both humans and animals [3 – 7]. These studies show histologically well marked improvement in tissue structure and, where investigated, significantly improved clinical findings. According to the currently available data, BCS improves the local metabolic environment inter alia by normalising cell physiology and reducing local oxygen radical formation. This allows local stem cells and macrophages to be active in tissue regeneration [8,9]. This property is also beneficial for acute and chronic joint injuries [10,11]. Post-operative treatment with BCS is also possible and significantly improves the outcome post ACL reconstruction [11].
Conclusion
BCS is effective in soothing the painful inflammatory process (as in the described case) and, unlike corticoids, initiates regeneration of the damaged tissue. As the maintenance of the structure and function of the rotator cuff is crucial to the health of the shoulder joint, local BCS infiltrations are available as a supplement to the indicated established treatments to achieve a rapid and reliable return to match fitness.
References
[1] Hardy et al. editors. The BMA guide to sports injuries. London: Dorling Kindersley; 2010
[2] Damjanov et al. PMID: 30167587
[3] von Wehren et al. PMID: 30900032
[4] Majewski et al. PMID: 19875360
[5] Genç et al. DOI: 10.1016/j.aott.2018.01.005
[6] Geburek et al. PMID: 26113022
[7] Wright Carpenter et al. PMID: 15532000 und PMID: 15532001
[8] Blázquez et al. PMID: 31316380
[9] Shirokova et al. PMID: 31847701
[10] Baltzer et al. PMID: 18674932
[11] Darabos et al. PMID: 21360125
Autoren

ist Facharzt für Orthopädie und Unfallchirurgie, Zusatzbezeichnungen Sportmedizin und Chirotherapie. Er ist Gründer und Leiter des interdisziplinären Ortho Zentrum HafenCity in Hamburg. Seit über 20 Jahren Betreuung von Kader- und Profisportler, u. a. 2001 – 2016 Mannschaftsarzt der Hamburg-Freezers in der DEL und 2004-2014 Feldhockey-Nationalmannschaft

ist Facharzt für Orthopädie & Unfallchirurgie mit Zusatzbezeichnung Sportmedizin und Chirotherapie am Orthozentrum HafenCity. Er ist Mannschaftsarzt der 1. Damen HTHC (HockeyBundesliga), Turnierarzt EHL (Euro Hockey League), Turnierarzt Beach-Volleyball-WM 2019, Kooperationspartner und Betreuung Nachwuchssport und Turnierarzt ATP Tennisturnier am Rothenbaum.


