
Physical therapies in sports medicine
We make far too little use of the possibilities offered by physical therapy in sports medicine. This statement was not made by us but by our scientific advisor, Robert Percy Marshall, MD, team physician for RB Leipzig. He made this statement during a presentation at DKOU 2024, and we at sportärztezeitung wholeheartedly agree. For this reason, we would like to introduce you to this exciting field in the following issues and also show you in a very concrete and practical way the potential and advantages of the various therapy methods, such as extracorporeal shock wave therapy.
The range of treatments includes cryotherapy (radial and focussed), neuro-reflective cryotherapy and heat therapy, laser therapy, electrotherapy, magnetic field applications, and magnetic resonance therapy. Peter Stiller gives a differentiated insight into the topic of cryotherapy on page 30 and in this context presentes the application of neuro-reflector hyperbaric CO2 cryotherapy paired with his experiences (www.sportaerztezeitung.com/rubriken/therpie/18072/cryotherapie/). Here you find an article by PD Anna Schreiner, MD on magnetic resonance therapy. What exactly is it, how does it relate to MRI, and how does it differ from magnetic field therapy? Supplemented by practical and application-oriented insights from the world of professional sport by Prof. Götz Welsch, MD (HSV). sportärztezeitung
Magnetic resonance therapy
Sports medicine and comprehensive conservative therapy should be broadly based, sensibly multimodal, ideally customised to the individual patient and open to new additions to the range of therapies. We sports physicians /doctors are on the right track, but we are nevertheless often confronted with a certain treatment gap, the desire for a more cause-orientated rather than purely symptom-orientated therapy and specialist training that does not always justice to this.
For historical reasons, physical therapy methods have been underestimated or only used to a limited extent in practice. In German-speaking countries, for example, magnetic resonance therapy (MBST®) or tNMR (therapeutic nuclear magnetic resonance) is little known despite many years of experience and (inter)national use. In addition to the often heterogeneous evidence-based medicine situation, the experience of the individual physician often plays a decisive role in determining therapeutic action, which for historical reasons – in addition to surgical methods – is predominantly characterised by interventions in chemical processes and less by the application of physical principles. Naturally, these in turn could only be investigated after recognising the scientific correlations at a molecular and cellular level and corresponding disorders could only be addressed after discovering the electrical processes in the living body. Most recently, the interdisciplinary field of quantum biology has developed from this [10].
This article sheds light on this therapeutic principle, which starts at the level of causal cell health, has a symptomatic effect, has enormous potential and positively modulates Nobel Prize-winning cell processes. In addition, previous areas of application – including professional sports – are shown and this is differentiated from other methods for orientation purposes.
Discovery, development & clinical use
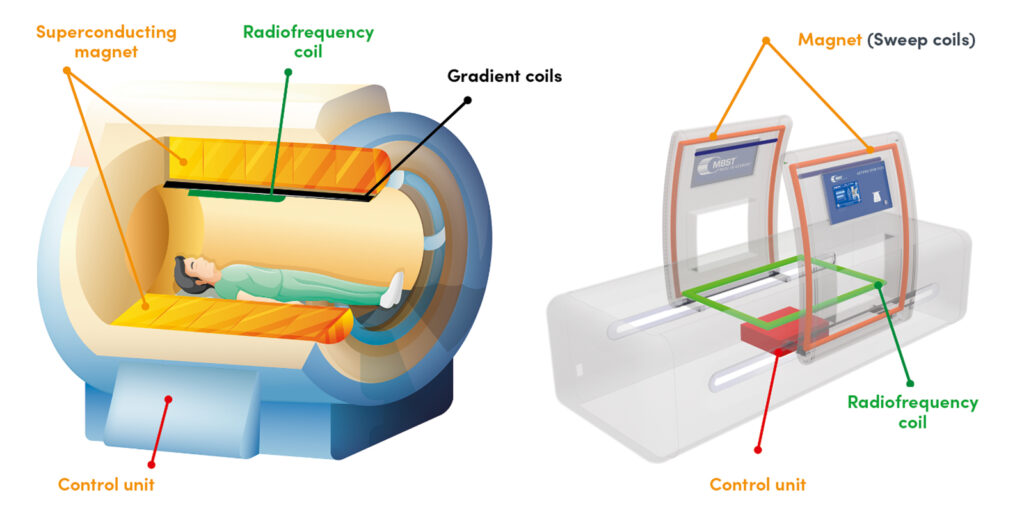
In the early days of MRI (magnetic resonance imaging), test subjects and patients often had to be examined repeatedly and with long examination times. It was discovered by chance that some patients reported health improvements afterwards, such as better mobility, more energy or less joint pain. The developers of the later MBST® technology became aware of these results and discovered that the positive effect at the cellular level was triggered by the energy transfer to protons in resonance [1]. However, years of interdisciplinary research and development work were required to be able to utilise magnetic resonance technology therapeutically, i. e. to achieve this effect without the complexity of MRI and to develop a widely usable therapy system. Relevant tissue parameters such as proton density, repetition and relaxation times were determined for different tissues (bone, cartilage, etc.), taking into account the corresponding Larmor frequency. This therapy is based on the same physical principles as MRI but operates at a much lower magnetic field strength and uses significantly lower radio (pulse) frequencies (RF) (see Fig. 1).
Magnetic resonance therapy has been in clinical use since 1998 and is a non-invasive, drug-free, and pain-free therapy option, either as an alternative or supplement. It is used by medical professionals to treat various indications and tissue types in the case of complaints, injuries and painful, degenerative and/or pathological changes to the musculoskeletal system. With regard to contraindications, MRI should be used as a guide. The devices (MBST®) are Class IIa medical devices and approved in accordance with EU 2017/745 Medical Device Regulation (MDR) and require therapy cards containing the tissue-specific software.
The physics behind it: Low magnetic fields and radiofrequency as efficient partners and differentiation from similar physical therapy methods
In nuclear magnetic resonance therapy (tNMR), the human body is not exposed to any harmful radiation. Instead, both MRI and tNMR devices use magnets and radio signals that measurably influence hydrogen protons in the body, which consists of approximately 70 % water, in the short term and – in contrast to the geomagnetic field – align them in a targeted manner for a limited period of time. The respective tNMR power parameters to establish nuclear magnetic resonance conditions with the target tissue, successive radio frequency impulses and to repeat the treatment parameters tissue-specifically depending on the phase are:
- Radio frequency power: max. 1 W at resonance
- Radio frequency range: 13.5 – 18 kHz
- Magnetic field strength: max. 1 mT
To generate nuclear magnetic resonance in tNMR, three coordinated fields of different properties are required: A static main magnetic field, a variable, long-modulated „sweep“ magnetic field parallel to the main magnetic field and an alternating electromagnetic field that satisfies the Larmor frequency condition (for hydrogen atoms) and must be perpendicular to the other fields. The output signals each contain a modulated, rectified magnetic field with a static component and a modulated alternating field.
The relevant effect for the treatment is the so-called Adiabatic Fast Passage (AFP). Put simply, energy is only transferred if the transmitter (MBST®) and receiver (tissue) have the same parameters, i. e. resonance conditions exist. This physical principle has been confirmed by scientific reports [1, 2].
The most common risk of confusion to date is with (so-called non-invasive) magnetic field therapies (MFT). Here, devices generate static or pulsating fields of various kinds. The frequency, the periodic change of direction and the intensity of the magnetic field can be individually adjusted. In contrast to tNMR, this is not a therapy that produces nuclear magnetic resonance based on the parameters, but rather a wide range of different magnetic fields with heterogeneous evidence. tNMR is a non-comparable and much more complex method compared to conventional MFT. In contrast to the ionic functional principle of MFT, in tNMR the energy transfer is carried out at the proton level of the hydrogen atoms in resonance. As the human body consists of almost 80 % water, energy can be optimally transferred into the tissue almost without loss via this route. tNMR is an independent, innovative and unique therapeutic procedure in terms of bio-physics. It is the only non-invasive method in the world that works directly at the hydrogen proton and therefore cell level.
Commercially available MFT devices mostly use the PEMF method (pulsed electromagnetic fields). These are fields that build up and break down. The magnetic field is located inside a thin-walled air coil, is strongest at the edge of the coil and decreases towards the centre. However, it does not have a core spin field or its properties. The devices are usually adjustable in terms of frequency, waveform and power and can be freely selected by the doctor or patient for home use. This PEMF technology, which is scientifically controversial in some quarters, is based on the transfer of energy into the organism through ion transport (ion level) via an air coil system with simple pulsing, i.e. switched on and off, magnetic fields (PEMF). This is intended to stimulate metabolic processes in the cell structures and support regeneration. However, only a small amount of energy is transferred to the organism in this way, as the form of energy transfer does not have a biological signal form and such air coil systems tend to have higher losses, which limits their effectiveness. These systems cannot cause resonance effects because they do not operate under Larmor conditions, which is a basic prerequisite for inducing resonance effects in cells and thus a demonstrable therapeutic effect. Only with tNMR, i.e. a combination of a static magnetic field, a sweep field and a radio frequency applied orthogonally to it, can proton spins be specifically stimulated.
In repetitive peripheral magnetic stimulation (rPMS), the nerves that control the muscles are stimulated and activated by magnetic pulses to relieve pain. Strong, rapidly pulsing magnetic fields are used to stimulate nerve cells and muscle fibres using the principle of induction. The rPMS device generates pulses at frequencies similar to those used by the body itself for neuromuscular control and regulation (5-50 Hz). In high-energy induction therapy, for example, a magnetic field is generated that is about 600 times stronger than a normal magnetic rod and can vary between 1-150 Hz. The pulses are noticeable to the patient and the clicking of the magnetic coil stimulation is audible.
In the field of alternative medicine, the use of mats is also known, whose mode of action consists of an electromagnetic field that is intended to address the functionality of capillaries by specifically intervening in the body’s bioelectrical processes. The devices sold by manufacturers such as BEMER Int. AG generate a very weak magnetic field of 50 to 100 µT, which corresponds approximately to the strength of the Earth’s magnetic field at the Earth’s surface.
Overall, static magnetic fields are well described in nature, whereas the heterogeneous study situation on pulsating magnetic fields using a wide range of frequencies cannot be generalised. The range of indications for MFT is broad and also includes orthopaedic and sports medicine.
Transcranial magnetic stimulation (TMS) is based on the law of electromagnetic induction. This states that an electric current is induced in a conductor when the magnetic flux changes, which in turn changes when the electric current in the magnetic coil generating the magnetic field changes. Technically, this is achieved by quickly switching the current in a magnetic coil on and off with the aid of a thyristor switch. This electrical current, which changes over time, induces a magnetic flux that also changes, which in turn induces an electrical current in the ‘conductor’ brain. In order to induce a magnetic flux change that reaches the cerebral cortex through the skin and bones, voltages of up to 2000 V and currents of up to 10,000 A are required. Accordingly, the devices place high demands on safety.
This must be distinguished from invasive MFT (electro-osteo-stimulation (EOS)). Here, the magnetic field is used to transmit electrical energy, while the effect is based on electrical stimulation, whereas in the non-invasive method, the magnetic field as such exerts its effect in the body.
Radio frequency therapy, on the other hand, is an invasive procedure used in the spinal area, e.g. for denervation. Here, heat is generated via radio waves (250 kHz to 1 MHz) (75–90 °C for 60–90 seconds). In pulsed radio frequency therapy, radio waves with a base frequency of approx. 500 kHz are used.
In the field of electrotherapy, a distinction is made between direct current therapy (galvanisation), low-frequency therapy (up to 1000 Hertz), medium-frequency therapy (1 to 100 kilohertz) and high-frequency therapy (over 100 kilohertz). Ultrasound therapy and TENS also belong to this group of therapeutic methods and are primarily used for symptomatic pain relief.
In summary, tNMR is a biophysically independent, innovative and unique therapeutic method. It is the only non-invasive method in the world that acts directly on hydrogen protons and thus at the cellular level.

Understanding the cellular level – Circadian cell clock and co.
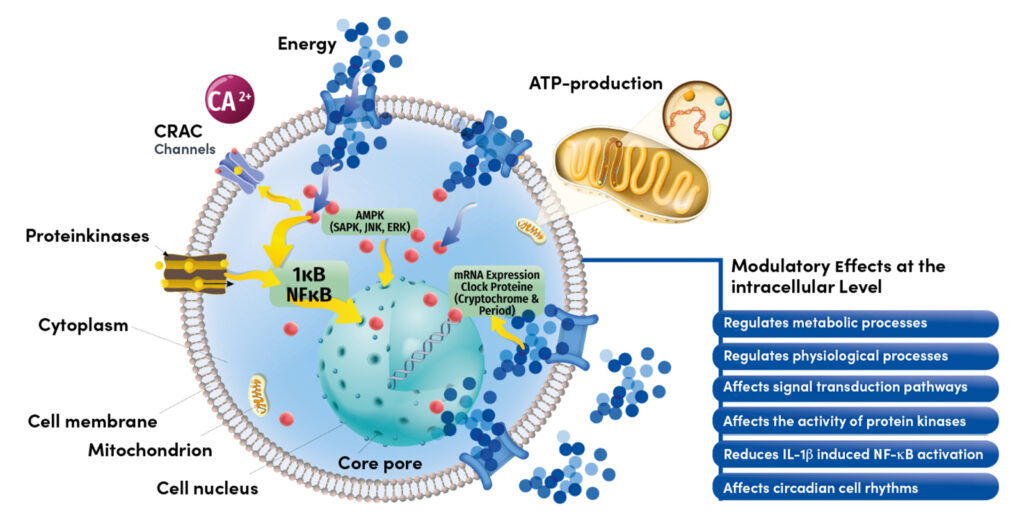
In order to understand why tNMR referred to as healing at the cellular level, is necessary to take a closer look at relationships that have so far been little known in everyday clinical practice. Living organisms are a highly complex biological system with numerous molecular, biochemical and bio-physical processes. Biological homeostasis is self-regulating and requires healthy cells. The body consists of cells and almost 80 % water (in tissue, cytoplasm, etc.). tNMR utilises the ubiquitous water protons in a tissue-specific manner and modulates various cell processes in the sense of homeostasis. An important aspect of cellular processes is the so-called circadian cell clock. This is an endogenous oscillation of metabolic activities with a periodicity of approx. 24 hours. All our cells in the body have such an internal clock, which consists of clock genes or proteins. The internal clock of the cells controls cellular signalling pathways such as the basal (sugar) metabolism, the mitochondrial respiration, immune and stress response or cell division. An „adjustment of the clock“ is associated with a variety of diseases [3 – 9]. tNRM has been shown to influence the cell clock [3, 10, 11]. In basic science tNMR studies, for example, it was shown that the combination of weak magnetic fields in combination with radio waves has a clear influence on the signalling pathways of the cell – such as the internal clock, the basic cell metabolism or the oxygen signalling pathway [11 – 13]. This means that tNMR also has a positive influence on the balance of free oxygen radicals [12]. These so-called ROS (reactive oxygen species) not only have a harmful effect if too much of them are formed, but are also necessary for the fine control of cellular signalling pathways. High ROS concentrations ultimately lead to irreparable damage to macromolecules and DNA and can trigger cell apoptosis. The findings on hypoxia-controlled signalling pathways were awarded the Nobel Prize in 2019 („When cells get out of breath“ – Kaelin, Ratcliffe, Semenza [14]) and are also described in connection with osteoarthritis and bone metabolism, for example [15, 16].
In addition to other in vitro studies showing that tNMR reduces inflammatory and catabolic mechanisms and stimulates anabolic effects (see also the arthrosis model) [17, 18], the Innsbruck research group has repeatedly demonstrated the connection between the circadian cell clock and the hypoxic signalling as described above [3, 11 – 13, 19, 20]. Ultimately, tNMR can be used as a kind of switch for the cellular clocks and thus the metabolism of both human and veterinary cells. In another study it was shown that tNMR accelerated the regeneration of dorsal root ganglia in vitro [21, 22]. In summary, tNMR can activate the body’s own natural repair mechanisms,
Musculoskeletal applications and clinical evidence
MBST® is widely used to treat osteoarthritis, osteoporosis, and both acute and chronic sports injuries. It is also applied postoperatively for optimised wound healing, back pain, and pain management (both analgesic and anti-inflammatory) [1]. In terms of tissue types and treatment areas, cartilage (cartilage damage, arthrosis), bones (bone oedema, osteoporosis), intervertebral discs (herniated discs, back pain), nerves (nerve damage, pain) and muscles / tendons / ligaments (sports injuries, overuse reactions) can be addressed. tNMR can be used both as a standalone therapy and, more importantly, as part of a modern multimodal treatment approach. There are numerous studies, including nearly 30 relevant publications on MBST®, covering both clinical and scientific research. This includes collaborations with universities, research institutions, clinics, and medical practices worldwide. No side effects or complications have been reported so far in in any of the applications and procedures to date. In addition to various other specialist publications, the relevant publications (in addition to the basic scientific data presented above) are retrospective, but also prospective, controlled clinical studies of varying quality. The following main statements, among others, were shown in various studies [1, 23]:
- Pain reduction in osteoporosis, fewer osteoporosis-related complaints, i.e. improved quality of life, increased bone density (qCT), increased bone formation markers, fracture risk reduction [1, 24 – 32]
- Significant medium to long-term pain reduction in osteoarthritis, improvement in quality of life and joint function, optimisation of degenerated cartilage structures (according to the Eckstein procedure) [1, 33 – 40] ; additive in-vitro: modulation of cartilage metabolism (see HIF1α, reduction of lactase level), modulation of IL-1β-induced inflammatory reactions, positive influence on chondrocytes / osteoblasts [41, 42]
- Long-term improvement of Back pain, longer-lasting rehabilitation effect, reduction in sick days [43 – 48]
- Part of the successful multimodal treatment of muscle injuries (see article in sportärztezeitung) [49].
Case reports and application data also cover the area of neuralgia (PNP, CRPS, fibromyalgia, etc.), wound healing disorders, osteo-necrosis and numerous applications for acute and chronic sports injuries (see also articles in the sportärztezeitung). The various device types are certified in accordance with the EU standard for medical devices (EU 2017/745 MDR), including a regular evaluation report on safety and efficacy, and MBST® has now been tried and tested in more than 2 million hours of therapy. There is also a mobile device version for the sports medicine sector. Sports physicians and team doctors from Bundesliga teams, top international teams and Olympic athletes are already using it successfully – currently in Germany, for example, at HSV (Prof. Götz Welsch, MD) and Basketball Löwen Braunschweig (Nico Fiedler, MD).
Outlook and summary
To summarise, it can be said that tNMR is a long-established and successful procedure that is increasingly emerging as a relevant partner for modern multimodal therapy in a patient-individualised multimodal setting, not least due to the latest basic scientific data and increasing national and international clinical experience in the professional sports sector and orthopaedics as a whole. The experiences of many colleagues and patients often describe magnetic resonance therapy as „the missing piece“ that can help to close a treatment gap. Further studies are underway to optimise the evidence base. Particularly in the case of chronic common diseases such as osteoporosis and arthrosis, this therapy may a be a meaningful option in view of the socio-economic situation. Basic research is also constantly being carried out to explore further mechanisms of action, optimise treatment approaches and further therapy. This is what sport is all about, „to get all the horsepower back on the road“, i. e. to enable a successful and efficient return-to-sports etc. or to generally help patients to recover, or at least to reduce symptoms and improve their quality of life. If we continue with the car analogy, MBST® can help optimise cellular function, much like fine-tuning an engine. However, the whole thing also needs the right fuel, i. e. nutrients, vitamins, trace elements etc. in the form of food, food supplements, supplements etc. The vehicle also needs to be moved, i.e. training in whatever form. If a targeted repair is required due to ageing, an accident or similar, further physical therapies, orthobiologics and, if necessary, interventional procedures are used.
Insights from professional sport
from Prof. Götz Welsch, MD
The time factor also plays an important role. How can I get a footballer back on the pitch as quickly and safely as possible? In addition to medical, physiotherapeutic or osteopathic treatment, we use a wide range of physical therapies for chronic or acute injuries in professional sport, as mentioned at the beginning of the article. These forms of therapy must complement each other sensibly with the aim of accelerating tissue regeneration. After 12 months of experience with magnetic resonance therapy (MBST) in the context of supporting a professional football team, this form of therapy has proven to be an extremely useful addition to a multimodal treatment spectrum. As part of the therapy concept for typical injuries and overuse injuries in professional football, the team doctors manage the rehabilitation processes together with the physiotherapists and rehab/athletic trainers. Physical forms of therapy play a key role here and are applied differently depending on the injury. MBST has now become a very important component. We use the „ARTHRO•SPIN•FLEX 2“ magnetic resonance therapy treatment device for the following indications:
- Chronic cartilage damage in the knee and hip joint
- Bone bruises / bone marrow oedema (acute or chronic)
- Muscle injuries (both contusions and overloads / DOMS, strains, fibre and bundle injuries)
- Acute joint injuries (ankle, knee, shoulder, etc.)
- Back pain, intervertebral disc pathologies, spondylolysis
- Post-operative
It can be seen that these indications include the majority of all sports injuries and overuse injuries that occur in a professional football team. Depending on the affected structure, the specific MBST tissue types (e.g. cards for cartilage / osteoarthritis, bones, tendons, muscles, ligaments, intervertebral discs) are used.
The aim of multimodal combination therapy is to initiate various regenerative processes and utilise them alongside or with each other. In this way, the self-healing process should be supported and, if necessary, accelerated. Among other things, the aim is to achieve a modulation and resolution of the inflammatory processes that take place as part of this healing process. At the cellular level, as described above, homeostasis should be established, cell permeability and mitochondrial activity should be increased (increased energy supply) and cell metabolism and protein synthesis should be activated. The aim is to improve microcirculation and stimulate the secretion of nutrients, growth hormones and stem cells are activated in the healing process.
Individual physical measures have an impact on different, complementary processes in this cascade and often enable faster and more intensive treatment, while at the same time accelerating regenerative processes. Depending on the pathology, MBST is used together with microcurrent, shockwave, deep heat, laser, but sometimes also together with pulsating magnetic field therapy. A major advantage of MBST is certainly its tissue specificity and the possibility of treating even very deeply localised or intra-osseous pathologies in a targeted manner.
While magnetic resonance therapy can achieve a time advantage in the healing process for acute injuries, it is a very effective addition to the therapeutic procedure for chronic processes (cartilage damage / osteoarthritis, inflammation of the pubic bone / tendon attachment tendinopathies) and bone marrow oedema, which is often difficult to treat.
The aforementioned device has been accepted extremely well as part of team care. The 60-minute therapy time is very well tolerated by the athletes and we also use this for parallel treatments, e.g. microcurrent or ionising oxygen therapy. This therapy is planned and scheduled by the physiotherapists in consultation with the team doctors.
Bibliography
1 Clinical Evaluation Report, 2022, (CE-TPL-01) gemäß MD Regulation (EU) 2017/745; fortfolgend CER
2 Gutachten Prof. Dr. P. Jakob, Physikalisches Institut der Universität Würzburg, Lehrstuhl für Experimentelle Physik 5, Mai 2005
3 https://www.schroedingerskatze.at/die-innere-uhr-der-zellen/
4 Egg M, Kietzmann T. Little strokes fell big oaks: The use of weak magnetic fields and reactive oxygen species to fight cancer. Redox Biol. 2025 Feb;79:103483. doi: 10.1016/j.redox.2024.103483. Epub 2024 Dec 24. PMID: 39729909; PMCID: PMC11733197
5 Pan X, Mota S, Zhang B. Circadian Clock Regulation on Lipid Metabolism and Metabolic Diseases. Adv Exp Med Biol. 2020;1276:53-66. doi: 10.1007/978-981-15-6082-8_5. PMID: 32705594; PMCID: PMC8593891
6 Sulli G, Lam MTY, Panda S. Interplay between Circadian Clock and Cancer: New Frontiers for Cancer Treatment. Trends Cancer. 2019 Aug;5(8):475-494. doi: 10.1016/j.trecan.2019.07.002. Epub 2019 Aug 3. PMID: 31421905; PMCID: PMC7120250.
7 Musiek ES, Holtzman DM. Mechanisms linking circadian clocks, sleep, and neurodegeneration. Science. 2016 Nov 25;354(6315):1004-1008. doi: 10.1126/science.aah4968. PMID: 27885006; PMCID: PMC5219881.
8 Dudek M, Swift J, Meng QJ. The circadian clock and extracellular matrix homeostasis in aging and age-related diseases. Am J Physiol Cell Physiol. 2023 Jul 1;325(1):C52-C59. doi: 10.1152/ajpcell.00122.2023. Epub 2023 May 29. PMID: 37246635; PMCID: PMC10281784.
9 Roenneberg T, Merrow M. The Circadian Clock and Human Health. Curr Biol. 2016 May 23;26(10):R432-43. doi: 10.1016/j.cub.2016.04.011. PMID: 27218855.
10 https://www.uibk.ac.at/de/newsroom/2022/durch-quantenbiologie-zu-neuen-therapieansatzen/
11 Thöni V, Dimova EY, Kietzmann T, Usselman RJ, Egg M. Therapeutic nuclear magnetic resonance and intermittent hypoxia trigger time dependent on/off effects in circadian clocks and confirm a central role of superoxide in cellular magnetic field effects. Redox Biol. 2024 Jun;72:103152. doi: 10.1016/j.redox.2024.103152. Epub 2024 Apr 5. PMID: 38593630; PMCID: PMC11016797.
12 Thöni V, Oliva R, Mauracher D, Egg M. Therapeutic Nuclear Magnetic Resonance affects the core clock mechanism and associated Hypoxia-inducible factor-1. Chronobiol Int. 2021 Aug;38(8):1120-1134. doi: 10.1080/07420528.2021.1910288. Epub 2021 Apr 13. PMID: 33847185.
13 Thöni V, Mauracher D, Ramalingam A, Fiechtner B, Sandbichler AM, Egg M. Quantum based effects of therapeutic nuclear magnetic resonance persistently reduce glycolysis. iScience. 2022 Nov 9;25(12):105536. doi: 10.1016/j.isci.2022.105536. PMID: 36444297; PMCID: PMC9700021.
14 https://www.aerzteblatt.de/archiv/nobelpreis-fuer-medizin-wenn-zellen-ausser-atem-kommen-3bded02a-58ff-454d-badf-f96bb794a606
15 Husa et al, Nat Med. 2010, Aro et al, JBC, 2012 Guo, H., Huang, J., Liang, Y. et al. Focusing on the hypoxia-inducible factor pathway: role, regulation, and therapy for osteoarthritis. Eur J Med Res 27, 288 (2022)
16 Maes, C., Carmeliet, G. & Schipani, E. Hypoxia-driven pathways in bone development, regeneration and disease. Nat Rev Rheumatol 8, 358–366 (2012). https://doi.org/10.1038/nrrheum.2012.36
17 Steinecker-Frohnwieser B, Lohberger B, Eck N, Mann A, Kratschmann C, Leithner A, et al. (2021). Nuclear Magnetic Resonance Therapy Modulates the Mirna Profile in Human Primary OA Chondrocytes and Antagonizes Inflammation in Tc28/2a Cells. Int. J. Mol. Sci. 22:5959.
18 Steinecker-Frohnwieser B, Kullich W, Mann A, Kress H.G., Weigl L. (2018) The therapeutic nuclear magnetic resonance changes the balance in intracellular calcium and reduces the interleukin-1induced increase of NF- activity in chondrocytes. Clin. Exp.Rheumatol. 2018, 36, 294–301
19 Oliva, R., Jansen, B., Benscheidt, F., Sandbichler, A. M., & Egg, M. (2018). Nuclear magnetic resonance affects the circadian clock and hypoxia-inducible factor isoforms in zebrafish. Biological Rhythm Research, 50(5), 739–757. https://doi.org/10.1080/09291016.2018.1498194
20 https://www.oulu.fi/en/news/switch-for-internal-clock-exploring-quantum-biology-for-novel-medical-therapies
21 Mann A, Steinecker-Frohnwieser B, Naghilou A, Millesi F, Supper P, Semmler L, Wolf S, Marinova L, Weigl L, Weiss T, Radtke C. Nuclear Magnetic Resonance Treatment Accelerates the Regeneration of Dorsal Root Ganglion Neurons in vitro. Front Cell Neurosci. 2022 Mar 28;16:859545. doi: 10.3389/fncel.2022.859545. PMID: 35418835; PMCID: PMC8995532.
22 Rad A, Weigl L, Steinecker-Frohnwieser B, Stadlmayr S, Millesi F, Haertinger M, Borger A, Supper P, Semmler L, Wolf S, Naghilou A, Weiss T, Kress HG, Radtke C. Nuclear Magnetic Resonance Treatment Induces ßNGF Release from Schwann Cells and Enhances the Neurite Growth of Dorsal Root Ganglion Neurons In Vitro. Cells. 2024 Sep 13;13(18):1544. doi: 10.3390/cells13181544. PMID: 39329728; PMCID: PMC11430304.
23 https://www.mbst.de/mbst-studien.php und s.a. CER
24 CER: Klapsch, 2003: Prospektive Untersuchung zur Wirksamkeit der MBST Kernspinresonanztherapie bei Ganzkörperbehandlung als mögliche nicht medikamentöse
Therapie bei Osteoporoseerkrankung
25 CER: Grumbrecht, 2003: MBST Kernspinresonanztherapie als mögliche nicht medikamentöse Therapie bei Osteoporose
26 CER: Handschuh et Melzer, 2008, Behandlung der Osteoporose mit der MBST Kernspinresonanztherapie, Sonderdruck ORTHODOC 05/2008
27 CER: Krpan et al., 2015: Therapeutische Anwendung der Kernspinresonanz bei Osteoporose
28 Krpan D, Kullich W. Nuclear magnetic resonance therapy (MBST) in the treatment of osteoporosis. Case report study. Clin Cases Miner Bone Metab. 2017 May-Aug;14(2):235-238. doi: 10.11138/ccmbm/2017.14.1.235. Epub 2017 Oct 25. PMID: 29263740; PMCID: PMC5726216.
29 CER: Krpan et al., 2017: Nuclear magnetic resonance therapy in osteoporosis reduces the risk of fractures in accidents/downfalls – case report study
30 Krpan D et al., Non-pharmacological treatment of osteoporosis with Nuclear Magnetic Resonance Therapy (NMR-Therapy), Periodicum biologorum, Vol 117, No 1, 161-165 2015
31 Krpan D. A new concept of integrated holistic approch in treatment of chronic musculoskeletal diseases The “BAR” method. Periodicum biologorum [Internet]. 2015 [pristupljeno 28.02.2025.];117(1):119-124. Dostupno na: https://hrcak.srce.hr/139530
32 CER: Overbeck et al., 2003: Scientific Evaluation of the Effectiveness of wholebody MBST® Nuclear Magnetic Resonance Therapy for Treatment of Osteoporosis
33 Froböse et al., 2000: Evaluation der Effektivität dreidimensionaler pulsierender elektromagnetischer Felder der MultiBioSignal-Therapie (MBST) auf die Regeneration von Knorpelstrukturen; Orthopädische Praxis, 8/2000, 36, 510-515
34 CER: Auerbach et al., 2003: Prospektive Untersuchung der Wirksamkeit der MBST®-Kernspinresonanztherapie bei der Behandlung der Gonarthrose
35 CER: Kullich et al., 2008: Funktionsverbesserung bei Fingergelenkarthrosen durch therapeutischen Einsatz der Kernspinresonanz
36 CER: Fagerer et al., 2007: Anwendung der Kernspinresonanz als neue Therapiemöglichkeit bei Gonarthrose
37 CER: van Laack et al., 2011: Analyse der Langzeitwirkung der MBST-Kernspinresonanztherapie bei Gonarthrose
38 Kullich W, Overbeck K, Spiegel HU. One-year-survey with multicenter data of more than 4,500 patients with degenerative rheumatic diseases treated with therapeutic nuclear magnetic resonance. J Back Musculoskelet Rehabil. 2013;26(1):93-104. doi: 10.3233/bmr-2012-00362. PMID: 23539765.
39 Schmidt JK, Debess JE, Møller L. Magnetic resonance therapy in the treatment of osteoarthritis: A scoping review. Radiography (Lond). 2021 Aug;27(3):968-975. doi: 10.1016/j.radi.2021.02.011. Epub 2021 Apr 11. PMID: 33853739.
40 Huels N, Harms O, Keim D, Rohn K, Fehr M. Treatment of the Clinical Symptoms of Osteoarthritis in the Elbow Joints of Dogs Using Nuclear Magnetic Resonance Therapy: A Randomized, Double-Blinded Trial. Front Vet Sci. 2020 Nov 13;7:500278. doi: 10.3389/fvets.2020.500278. PMID: 33282923; PMCID: PMC7691575.
41 Steinecker-Frohnwieser et al., The Influence of Nuclear Magnetic Resonance Therapy (NMRT) and Interleukin IL1-b Stimulation on Cal 78 Chondrosarcoma Cells and C28/ I2 Chondrocytes, J Orthopedics Rheumatol, May 2014, Vol 1, Issue 3
42 Temiz-Artmann A, Linder P, Kayser P, Digel I, Artmann GM, Lücker P. NMR in vitro effects on proliferation, apoptosis, and viability of human chondrocytes and osteoblasts. Methods Find Exp Clin Pharmacol. 2005 Jul-Aug;27(6):391-4. doi: 10.1358/mf.2005.27.6.896831. PMID: 16179956.
43 Salfinger H, Salomonowitz G, Friedrich KM, Hahne J, Holzapfel J, Friedrich M. Nuclear magnetic resonance therapy in lumbar disc herniation with lumbar radicular syndrome: effects of the intervention on pain intensity, health-related quality of life, disease-related disability, consumption of pain medication, duration of sick leave and MRI analysis. Eur Spine J. 2015 Jun;24(6):1296-308. doi: 10.1007/s00586-014-3601-7. Epub 2014 Oct 18. PMID: 25326180.
44 Kullich, W. & Schwann, H. & Machreich, K. & Ausserwinkler, M.. (2006). Additional outcome improvement in the rehabilitation of chronic low back pain after nuclear resonance therapy. Rheumatologia. 20. 7-12.
45 Kullich W, Schwann H, Walcher J, Machreich K. The effect of MBST®-NuclearResonanceTherapy with a complex 3-dimensional electromagnetic nuclear resonance field on patients with Low Back Pain. Journal of Back and Musculoskeletal Rehabilitation. 2006;19(2-3):79-87. doi:10.3233/BMR-2006-192-307
46 Salomonowitz G, Salfinger H, Hahne J, Friedrich M. Effekte der Kernspinresonanztherapie auf Krankenstand bei Patienten mit Nervenwurzelirritation infolge eines lumbalen Bandscheibenvorfalls [Impact of magnetic resonance therapy on sickness absence of patients with nerve root irritation following a lumbar disc problem]. Z Orthop Unfall. 2011 Oct;149(5):575-81. German. doi: 10.1055/s-0031-1280121. Epub 2011 Oct 7. PMID: 21984428.
47 Jinho Lee, In-Hyuk Ha, Me-riong Kim, Hyun-Woo Cho, Ji Yeon Seo, Hee-seung Choi, Kwang Chan Song, Byung-Cheul Shin, Joon-Shik Shin, Yoon Jae Lee, Pain, disability, and MRI changes in lumbar disc herniation patients treated with integrative medicine: Ten-year results of an observational study, Integrative Medicine Research, Volume 11, Issue 2, 2022, 100833, ISSN 2213-4220, https://doi.org/10.1016/j.imr.2022.100833.
48 https://sciup.org/vozmozhnosti-mbst-vozdejstvija-kak-monoterapii-hronicheskoj-dorsalgii-14918540-en#:~:text=The%20aim%3A%20to%20analyze%20the%20clinical%20effect%20of,by%20degenerative%20dystrophic%20changes%20of%20vertebral%20column%20structures.
49 CER: Toussaint, 2011: Spitzenmedizin im Handball – Bessere Versorgung durch kombinierten Einsatz verschiedener Therapien bei akuten Muskelverletzungen; und s.a. weitere Fallberichte Sportärztezeitung
50 Viktoria Thöni, Abriana Buchter, Andreas Flarer, Justin Lampe, Cordula Schlegel, and Margit Egg „Understanding therapeutic nuclear magnetic resonance (tNMR): splitting of components indicates its unique efficacy“, Proc. SPIE 13340, Quantum Effects and Measurement Techniques in Biology and Biophotonics II, (26 February 2025); https://doi.org/10.1117/12.3056086
Autoren

» Fachärztin für Orthopädie und Unfallchirurgie
» Chief Medical Officer, MBST Global, MedTec Medizintechnik GmbH
» Eberhard Karls Universität Tübingen + AKAD University
(Stand 2026)

ist Facharzt für Orthopädie und Unfallchirurgie und ärztlicher Leiter des UKE Athleticum am Universitätsklinikum Hamburg Eppendorf. Er hat seit 2021 eine Professur für Orthopädische Sportmedizin am UKE. Außerdem ist er leitender Mannschaftsarzt der HSV Fußball AG. Sein klinischer Fokus liegt im Bereich der regenerativen Knorpeltherapie, der Behandlung von Sportverletzungen und Überlastungsschäden. Prof. Welsch ist wiss. Beirat der sportärztezeitung.


