
Lateral ligament injuries of the upper ankle joint (OSG) are one of the most common ligament injuries of the musculoskeletal system and particularly affect people who are active in sports. Although lateral ligament ruptures often lead to persistent instability, post-traumatic osteoarthritis, and significant impairment of athletic performance if treated inadequately, this lesion is often considered a “minor injury” by both those affected and those treating them. Data show that only about half of all those affected undergo further diagnostic testing after an OSG sprain [1].
Prevalence, injury patterns, and clinical relevance
The incidence of lateral ankle sprains in the general population is approximately one injury per 10,000 people per day, with the lateral ligament structure affected in 85 % of cases. Young adults aged 15 – 35 are particularly affected. This rate is significantly higher in physically active populations, particularly in sports with a high jumping and pivoting load profile, such as basketball, handball, volleyball, and soccer [2 – 4]. The classic injury pattern, consisting of a combination of supination / inversion trauma with combined plantar flexion, often leads to a tear of the lateral capsular ligament apparatus at the upper ankle joint (USG). The most common injury (approx. 85 %) is to the anterior talofibular ligament (ATFL), followed by the calcaneofibular ligament (CFL) (52 – 75%) and, less frequently (< 10 %), the posterior talofibular ligament (PTFL).
The lateral capsular ligament apparatus of the OSG not only serves as a stabilizer against anterior talar translation and inversion in the upper ankle joint. The anterior and posterior fibulotalar ligaments, together with the anterior and posterior portions of the deltoid ligament, form a firm ligamentous ring in the transverse plane of the malleolar fork (Fig. 1). Injury to the lateral structures thus leads to complex rotational instability. Epidemiological data show that 20 – 40 % of patients develop persistent symptoms such as pain, impingement syndromes, and functional and structural chronic instabilities after initial ankle sprain [5]. In athletes, a recurrence rate of up to 34 % has been reported if no targeted neuromuscular and proprioceptive rehabilitation is performed [6]. The risk of a repeat ankle injury is five times higher after a lateral ligament rupture [7]. Long-term clinical studies show that even seemingly “simple” lateral ligament ruptures significantly increase the risk of post-traumatic ankle osteoarthritis, especially in cases of residual instability or incomplete rehabilitation. Microinstabilities and repeated subtle sprains lead to chondral damage, which can result in degenerative joint destruction [5, 6].
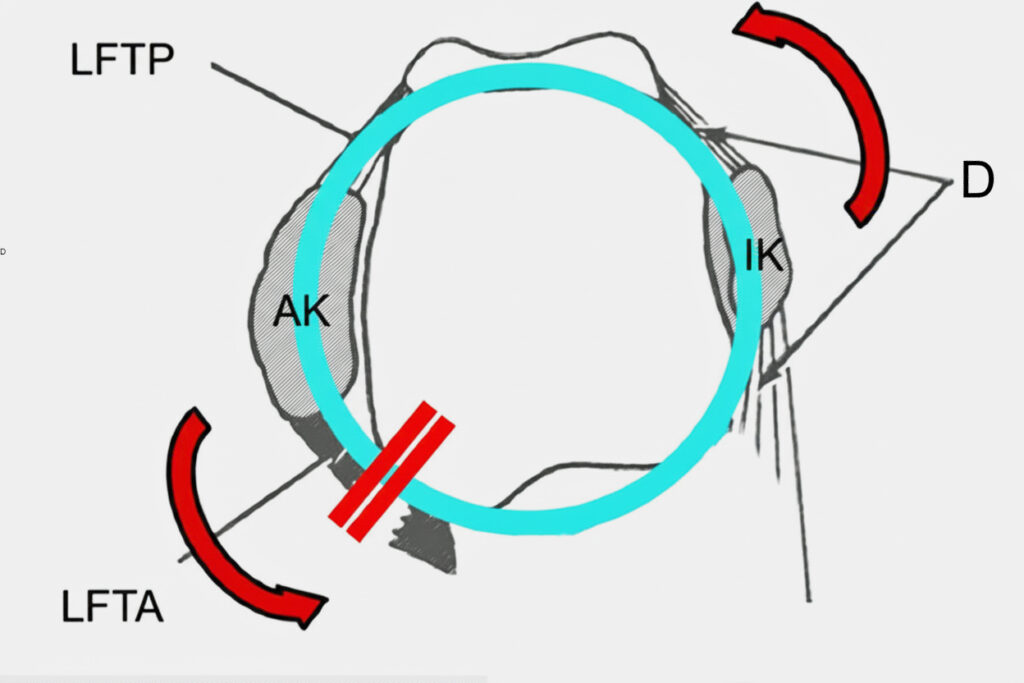 Fig. 1 Transverse view of the upper ankle joint. The deltoid ligament (D) forms a stable ligamentous ring together with the posterior tibiofibular ligament (PTL) and anterior tibiofibular ligament (ATFL) (LLC = lateral malleolus, MLC = medial malleolus). Rupture of the LFTA leads to a break in continuity with rotational instability in the upper ankle joint.
Fig. 1 Transverse view of the upper ankle joint. The deltoid ligament (D) forms a stable ligamentous ring together with the posterior tibiofibular ligament (PTL) and anterior tibiofibular ligament (ATFL) (LLC = lateral malleolus, MLC = medial malleolus). Rupture of the LFTA leads to a break in continuity with rotational instability in the upper ankle joint.
Diagnosis
Clinical examination forms the basis of the diagnosis. Targeted systematic palpation of the typical pain points (LFTA, LFC, anterior syndesmosis, peroneal tendons), the anterior drawer test, and the talar tilt test (inversion test) are used to test mechanical joint stability. Immediately after the acute event, swelling, pain, and muscle guarding significantly limit the informative value of these tests. A reevaluation after 3 – 4 days, as advocated by Niek van Dijk, enables a much more reliable assessment with improved diagnostic sensitivity and specificity [8].
Conventional X-ray diagnostics are not indicated if a fracture is not suspected. In particular, static images of the ankle joint do not provide reliable information in the acute injury situation. Ultrasound has proven to be a diagnostic tool for imaging ligament continuity, hematoma extent, and joint effusion volumes. Radiological studies have shown that the sensitivity of sonographic examination is significantly higher than that of MRI for imaging ruptured LFTA (94 – 100 vs. 67 – 87) and LFC (94 vs. 40 – 47) [9]. The specificity is approximately equivalent. Ultrasound thus enables rapid and cost-effective confirmation of the diagnosis and prompt initiation of treatment. Magnetic resonance imaging (MRI) remains indicated in cases of complex injury patterns, suspected concomitant pathologies such as osteochondral talus lesions, syndesmotic injuries, or in the absence of clinical improvement [10].
Conservative therapy and functional treatment concept
According to S2k guideline 187 – 025, conservative therapy is considered the gold standard for lateral ligament rupture without accompanying injury, provided that there are no complete ruptures of all three lateral ligaments with pronounced mechanical instability.
The main therapeutic goals are rapid pain reduction, edema reduction, restoration of physiological joint mobility, and regaining active-dynamic stability while minimizing the recurrence rate. Instead of complete immobilization and relief, early functional therapy with a semi-rigid ankle orthosis, which limits inversion and supination and reduces plantar flexion, is considered the standard. Several studies show that early functional treatment with early mobilization in the orthosis, full weight-bearing after pain and swelling have subsided, and accompanying physical therapy leads to a significantly faster return to sport, less muscle atrophy, and less joint stiffness than prolonged immobilization [11, 12]. Modular ankle orthoses have been available on the market for several years. The underlying concept of this treatment is the gradual reduction of the orthosis’s stabilization from the acute stage to the rehabilitation phase, adapted to the ligament healing phases. Modular systems allow for initially higher lateral guidance in the acute phase with a gradual reduction in stability over time, which supports early functional mobilization while protecting against renewed inversion trauma. This is intended to support improved alignment of the collagen fibrils in the regenerated tissue as well as improved proprioceptive stimulation [13].
Proprioceptive and neuromuscular training – the focus of recurrence prevention
Proprioceptive and neuromuscular training is the most essential component of rehabilitation, as functional instability is not exclusively structural, but is also caused by disturbed afferent feedback and delayed peripheral muscle response patterns. Randomized controlled trials (RCTs) [3, 12, 14, 15] show that 8-12-week progressive proprioceptive programs (wobble board, balance pad, standing on one leg on unstable surfaces) reduce the recurrence rate of sprains by 35 – 41 % and significantly improve functional stability scores. Meta-analyses [16, 17] of more than 30 RCTs combined show a significant reduction in the risk of re-rupture by 39 – 47 % through structured sensorimotor training (level 1a evidence). The S2k guideline 187 – 025 recommends starting proprioceptive training as early as week 2 – 3 after the trauma, i.e., already in the orthotic treatment phase, with a progressive increase until week 12. The focus is on balance exercises, agility skills, reactive changes of direction, and sport-specific jump-landing sequences for high-level athletes. Effective exercises include standing on one leg on an unstable surface, the Star Excursion Balance Test (Fig. 2), lateral hop tests, and multidirectional jumps with defined landing patterns [18].

Biological regenerative adjuvants: PRP, hyaluronic acid, and ESWT
The use of platelet-rich plasma (PRP) in ligament ruptures aims to increase local growth factor concentrations to optimize ligament healing. Initial clinical studies report some positive effects on pain and subjective stability [19 – 21]. However, the current data are heterogeneous. Large-scale RCTs specifically on acute lateral OSG ligament ruptures are limited. The S2k guideline did not issue a strong recommendation for PRP in acute ligament injuries. Hyaluronic acid injections are mainly used to modulate intra-articular inflammatory processes in soft tissue after an outer ligament rupture. Individual studies report faster pain reduction and a quicker return to sports [21, 22]. There is currently no consistent evidence of a benefit in accelerating ligament healing or reducing recurrent instability. At most, a complementary role may be considered in cases of associated chondral lesions. Preclinical models have demonstrated improved ligament regeneration, angiogenesis, and matrix remodeling with extracorporeal shock wave therapy (ESWT). No clinical data are available for this therapeutic measure in acute lateral ligament rupture, so there is no evidence-based recommendation. ESWT can be used as a selective option for reducing pain and swelling.
Conclusion
Consistent early functional therapy with adequate 6-week orthotic treatment, structured physical therapy, and intensive proprioceptive training form the main pillars of treatment. Proprioceptive training in the early phase and after removal of the orthosis is an essential factor in preventing functional instability and re-rupture.
Literature
- Vuurberg G, Hoorntje A, Wink LM, van der Doelen BFW, van den Bekerom MP, Dekker R, van Dijk CN, Krips R et al. Diagnosis, treatment and prevention of ankle sprains: update of an evidence-based clinical guideline. Br J Sports Med 2018, 52(15); doi: 10.1136/bjsports-2017-098106
- Junge A, Engebretsen L, Mountjoy ML, Alonso JM, Renström PA, Aubry MJ, Dvorak J.Sports injuries during the Summer Olympic Games 2008. Am J Sports Med 2009, 37(11):2165-72; doi: 10.1177/0363546509339357
- Doherty C, Delahunt E, Caulfield B, Hertel J, Ryan J, Bleakley C. The incidence and prevalence of ankle sprain injury: a systematic review and meta-analysis of prospective epidemiological studies. Sports Med 2014, 44(1):123-40. doi: 10.1007/s40279-013-0102-5
- van den Bekerom MP, Kerkhoffs GM, McCollum GA, Calder JD, van Dijk CN.Management of acute lateral ankle ligament injury in the athlete. Knee Surg Sports Traumatol Arthrosc 2013, 21(6):1390-5. doi: 10.1007/s00167-012-2252-7
- Valderrabano V, Hintermann B, Horisberger M, Fung TS.Ligamentous posttraumatic ankle osteoarthritis. Am J Sports Med. 2006, 34(4):612-20. doi: 10.1177/0363546505281813
- van Rijn RM, van Os AG, Bernsen RM, Luijsterburg PA, Koes BW, Bierma-Zeinstra SM.What is the clinical course of acute ankle sprains? A systematic literature review. Am J Med 2008, 121(4):324-331.e6. doi: 10.1016/j.amjmed.2007.11.018
- McKay GD, Goldie PA, Payne WR, Oakes BW.Ankle injuries in basketball: injury rate and risk factors. Br J Sports Med 2001, 35(2):103-8. doi: 10.1136/bjsm.35.2.103
- van Dijk CN, Lim LS, Bossuyt PM, Marti RK. Physical examination is sufficient for the diagnosis of sprained ankles. J Bone Joint Surg Br 1996, 78(6):958-62. doi: 10.1302/0301-620x78b6.1283
- Gribble PA.Evaluating and Differentiating Ankle Instability. . J Athl Train 2019, 54(6):617-627. doi: 10.4085/1062-6050-484-17. Epub 2019 Jun 4
- Crema MD, Krivokapic B, Guermazi A et al. MRI of ankle sprain: the association between joint effusion and structural injury severity in a large cohort of athletes Eur Radiol 2019, 29(11):6336-6344. doi: 10.1007/s00330-019-06156-1
- Kerkhoffs GM, Rowe BH, Assendelft WJ, Kelly K, Struijs PA, van Dijk CNImmobilisation and functional treatment for acute lateral ankle ligament injuries in adults. . Cochrane Database Syst Rev 2013, 28(3): CD003762. doi: 10.1002/14651858.CD003762
- Rivera MJ, Winkelmann ZK, Powden CJ, Games KE.Proprioceptive Training for the Prevention of Ankle Sprains: An Evidence-Based Review J Athl Train 2017, 52(11):1065-1067. doi: 10.4085/1062-6050-52.11.16
- Best R, Böhle C, Schiffer, T, Petersen W, Ellermann A, Brüggemann GP, Liebau C. Early functional outcome of two different orthotic concepts in ankle sprains: a randomized controlled trial. Arch Orthop Trauma Surg 2015, 135(7):993-1001. doi: 10.1007/s00402-015-2230-x
- Grimm NL, Jacobs JC Jr, Kim J, Amendola A, Shea KG.Ankle Injury Prevention Programs for Soccer Athletes Are Protective: A Level-I Meta-Analysis. J Bone Joint Surg Am 2016, 98(17):1436-43. doi: 10.2106/JBJS.15.00933
- Emery CA, Owoeye OBA, Räisänen AM, Befus K, Hubkarao T et al. The „SHRed Injuries Basketball“ Neuromuscular Training Warm-up Program Reduces Ankle and Knee Injury Rates by 36% in Youth Basketball. J Orthop Sports Phys Ther 2022, 52(1):40-48. doi: 10.2519/jospt.2022.10959
- van der Wees PJ, Lenssen AF, Hendriks EJ, Stomp DJ, Dekker J, de Bie RA.Effectiveness of exercise therapy and manual mobilisation in ankle sprain and functional instability: a systematic review. Aust J Physiother 2006, 52(1):27-37. doi: 10.1016/s0004-9514(06)70059-9
- Otsuka S, Papadopoulos K, Bampouras TM, Maestroni L.What is the effect of ankle disk training and taping on proprioception deficit after lateral ankle sprains among active populations? – A systematic review. J Bodyw Mov Ther 2022, 31:62-71. doi: 10.1016/j.jbmt.2022.04.001
- VBG Fachwissen. Return-to-Competition. Testmanual zur Beurteilung der Spielfähigkeit nach akuter lateraler Bandverletzung am Sprunggelenk. Stand Juni 2022. https://www.vbg.de/cms/sport/return-to-competition/rtc-sprunggelenk
- Ding Q, Wang X, Liu Y, Li Y, Zhang D, Wang H, Ma S, Han Q, Zhuang W.The efficacy of platelet-rich plasma in ankle disease: a systematic review and meta-analysis. . J Orthop Surg Res 2024, 31;19(1):895. doi: 10.1186/s13018-024-05420-5.
- Zhang J, Wang C, Li X, Fu S, Gu W, Shi Z.Platelet-rich plasma, a biomaterial, for the treatment of anterior talofibular ligament in lateral ankle sprain. . Front Bioeng Biotechnol. 2022, 22(10):1073063. doi: 10.3389/fbioe.2022.1073063
- Chen YT, Wu WT, Lee RP, Yu TC, Chen IH, Yeh KT.Platelet-rich plasma and hyaluronic acid in the treatment of acute ankle sprains: A review. Biomol Biomed 2025. doi:10.17305/bb.2025.13327.
- Petrella RJ, Petrella MJ, Cogliano A.Periarticular hyaluronic acid in acute ankle sprain. Clin J Sport Med 2007, 17(4):251-7. doi: 10.1097/JSM.0b013e3180f6169f
Autoren

» Fachärztin für Orthopädie und Unfallchirurgie sowie zertifizierte Fußchirurgin
» Leiterin Fußzentrum Helios Klinikum Hildesheim & Fußspezialistin Hannover, Privatpraxis für Fuß- und Sprunggelenkchirurgie
» Ehem. Präsidentin und Ehrenbeirat der Gesellschaft für Fuß- und Sprunggelenkchirurgie e.V. (GFFC)
(Stand 2026)


