
Apophyses are so-called ‘secondary ossification centres’ at the insertion sites of muscle tendons and do not fully mature until the end of the second decade of life (puberty) [14]. Even before the bony fusion with the adjacent bone, they are subject to high tensile and bending forces, especially during intensive training, and are therefore very vulnerable to injury [1, 15 – 17].
Sports such as football, which involve a lot of sprinting and quick changes of direction or jumping with high muscle tension, are considered high-risk sports [16]. Although various factors are discussed in the context of puberty as possible causes, such as individual growth compared to peers, hormonal status and changes in biomechanical and neuromotor conditions [5 – 7], training load is a plausible treatment-relevant factor, especially for young footballers. Regular and intensive training can lead to overuse injuries in the form of repetitive microtraumas and in some cases even cause a complete tear, a so-called avulsion fracture. Avulsion fractures are rare, but their prevalence, especially in adolescent males, is significantly higher than in mature athletes [2]. Overuse injuries account for up to 40 % of all absences from youth football [18, 19]. In a study of almost 550 young footballers in the age groups U9–U19 and an observation period of four seasons, injuries to the growth plates (epiphysis and apophysis) were recorded as the most common reason for injury-related training absences in young professional football, along with contusions and sprains [2]. Avulsion fractures are often underestimated and inadequately treated, which, especially in professional football, can have not only sporting but also economic consequences for the athlete and the club, and in the worst case can even mean the end of the career.
Diagnostics
Athletes often describe a sudden shooting pain in the transition area from the buttock to the back of the thigh when sprinting or changing direction abruptly. This is already crucial for an initial assessment. Meanwhile, in most youth development centres, video material from training sessions or match days can be accessed via the match analysis department, which can help to understand the mechanism of the accident. Clinically, pressure pain in the area of the ischial tuberosity (lat.= tuber ischiadicum) and the adjacent insertion of the hamstring tendon complex (so-called conjoint tendon) is characteristic. Pain during active knee flexion or hip extension from a prone position, with or without reduced strength (side-by-side comparison), are also typical findings. Clinical manual examination is an important part of the daily physiotherapy treatment with the athlete and helps to recognise injuries in time and treat them accordingly, even in the overuse stage. In close consultation with the athletic director, adjustments to training loads are necessary when dealing with overuse reactions in the muscle tendon area and are often crucial to avoid long periods of downtime. Hypoechogenic areas in the tendon transition or irregular cartilage-bone transitions on ultrasound can provide initial indications of a structural injury. In particular, newer portable ultrasound models enable initial imaging findings to be made at the site of the injury. Due to the increase in general sporting activity in the population in recent years and the better understanding of sports-related injuries, it is recommended that MRI diagnostics be used more extensively, especially in junior competitive sports. Therapy-relevant diagnostic details and accompanying pathologies, in particular the vulnerable growth plates, can be visualised in detail in MRI, even when conventional X-rays do not show an avulsion fracture in most cases.
Therapy
Treatment is generally conservative and includes partial weight-bearing on crutches and limited hip flexion with combined knee extension. After six weeks, rehabilitation can begin with active range-of-motion exercises and careful muscle building. Full clearance for sports should always be given when the patient is pain-free and has fully recovered range of motion (ROM) and equal leg strength. According to current literature, almost 80 % of patients treated conservatively heal successfully, although there is a complication rate of up to 30 % [9]. Pseudarthrosis is a typical complication. Persistent symptoms and a strength deficit on one side compared to the other, even after more than 6 weeks, may indicate an impaired healing process, as in the case study presented here. Various studies in recent years show a trend, particularly in athletes, to treat fractures with a displacement of ≥ 1.5 cm surgically in order to achieve primary stability and avoid complications and long periods of inactivity [10 – 13].
Case study
A 16-year-old up-and-coming professional footballer presented with complaints in the posterior thigh / buttock area that had been present for four months. Initially, he had experienced a sudden shooting pain in the posterior thigh while challenging for the ball. Since then, he had experienced pain dependent on loading and a significant reduction in strength. Initially assessed as a ‘muscle strain’, a three-week break from training and several sessions of physiotherapy were prescribed. However, a pain-free return to full training could not be achieved. Clinically, there was an increased basal tone of the hamstring muscles and pressure pain at the ischium near the insertion point.
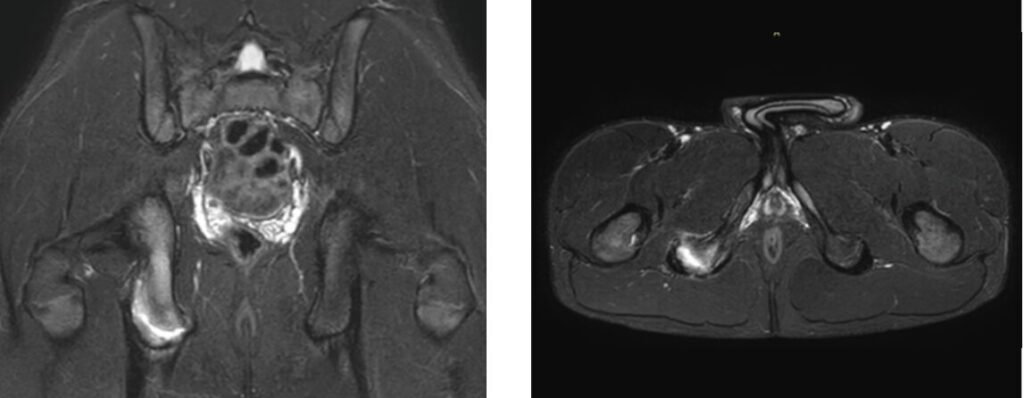
In the mobility test, hip flexion with an extended knee led to pain at the iliac hamstring tendon insertion point even at 70 °. The subsequent X-ray (Fig. 1) showed an avulsion fracture with complete detachment of the apophysis on the right ischium with incipient callus formation. The MRI of the pelvis (Fig. 2 a + b) clearly showed the avulsion with pronounced oedema in the fracture gap. The tendon insertion on the fragment appeared to be intact. The findings were discussed in detail with the parents and surgical treatment was indicated.

Surgical procedure and follow-up treatment
The patient was placed in a prone position with the leg free to move. Access was gained via an approximately 8 cm long horizontal skin incision centred at the level of the gluteal fold. After opening the fascia, the fracture and the tendon insertion area were exposed and visualised, with extensive separation of the surrounding scar tissue of the surrounding scar tissue. The proximal parts of the hamstring tendon were also separated from the scar tissue for later repositioning. Then the fragment was completely detached from the ischium. The fracture ends were freshened up with the sharp spoon, reduced using reduction forceps and fixed with a Kirschner wire. After reduction control under image intensifier – fluoroscopy, the fragment was fixed with 2 small fragment screws of approx. 30 mm length (Fig. 3 a + b). The hamstring tendon was also fixed to the remaining ischial tendon portion using FibreWibre® (FA Arthrex). When moving the leg, stable osteosynthesis and normal tendon tension were observed. After extensive rinsing and insertion of a drain, the wound was closed in layers. The follow-up treatment was early functional without orthosis and with partial weight-bearing (15 kg) on crutches for six weeks. The postoperative course was uncomplicated with close follow-up examinations. The X-ray check after six weeks (Fig. 4) showed timely fracture consolidation, so that a transition to full weight-bearing was possible. Further increases in load were carried out step by step and in close consultation with the team of physiotherapists in the rehabilitation department. The patient was only allowed to return to football-specific training after twelve weeks and when his leg strength was equal on both sides (isokinetic strength measurement).
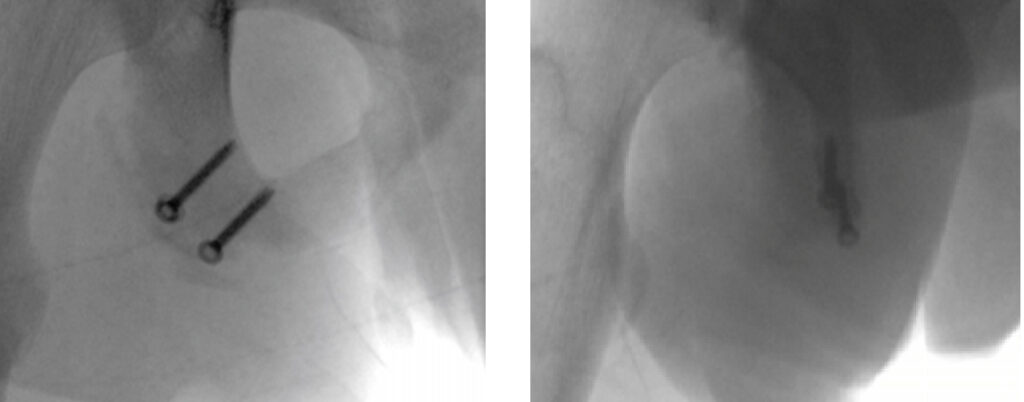 Fig. 3 a + b Intraoperative image intensifier control after repositioning and osteosynthesis with two small fragment screws and a washer.
Fig. 3 a + b Intraoperative image intensifier control after repositioning and osteosynthesis with two small fragment screws and a washer.

Conclusion
- Avulsion fractures of the pelvis are typical sports injuries, especially in young boys playing football
- Overuse injuries are among the most common reasons for a loss in youth football
- Overuse-associated apophysitis or tendinitis can lead to a traumatic avulsion fracture if inadequately treated in athletes and should therefore be investigated at the first clinical signs (pelvic attachment pain)
- MRI diagnostics is the gold standard and should be performed in adolescents at the slightest suspicion of apophysis involvement
- In most cases, therapy can be conservative, but patients with high athletic aspirations, especially professional athletes, should be treated surgically if the dislocation is ≥ 1.5 cm.
Bibliography
- Arnaiz, J., et al., Imaging findings of lower limb apophysitis. AJR Am J Roentgenol, 2011. 196(3): p. W316-25.
- Materne, O., et al., Injury incidence and burden in a youth elite football academy: a four-season prospective study of 551 players aged from under 9 to under 19 years. Br J Sports Med, 2021. 55(9): p. 493-500.
- Pogliacomi, F., et al., Anterior iliac spines fractures in the adolescent athletes: Surgical or conservative treatmentì. Medicina dello Sport, 2013. 66: p. 231-240.
- Rossi, F. and S. Dragoni, Acute avulsion fractures of the pelvis in adolescent competitive athletes: prevalence, location and sports distribution of 203 cases collected. Skeletal Radiology, 2001. 30(3): p. 127-131.
- Davis, K.W., Imaging pediatric sports injuries: lower extremity. Radiol Clin North Am, 2010. 48(6): p. 1213-35.
- Longo, U.G., et al., Apophyseal injuries in children’s and youth sports. Br Med Bull, 2016. 120(1): p. 139-159.
- Micheli, L.J. and A.F. Fehlandt, Jr., Overuse injuries to tendons and apophyses in children and adolescents. Clin Sports Med, 1992. 11(4): p. 713-26.
- Moeller, J.L., Pelvic and hip apophyseal avulsion injuries in young athletes. Curr Sports Med Rep, 2003. 2(2): p. 110-5.
- Di Maria, F., et al., Treatment of avulsion fractures of the pelvis in adolescent athletes: A scoping literature review. Frontiers in Pediatrics, 2022. 10.
- Biedert, R.M., Surgical Management of Traumatic Avulsion of the Ischial Tuberosity in Young Athletes. Clinical Journal of Sport Medicine, 2015. 25(1): p. 67-72.
- Cai, W., Y. Xie, and Y. Su, Comparison of non-surgical and surgical treatment using absorbable screws in anterior-superior iliac spine avulsion fractures with over 1.5cm displacement. Orthopaedics & Traumatology: Surgery & Research, 2020. 106(7): p. 1299-1304.
- Ferlic, P.W., et al., Treatment for ischial tuberosity avulsion fractures in adolescent athletes. Knee Surg Sports Traumatol Arthrosc, 2014. 22(4): p. 893-7.
- Li, X., et al., Results of operative treatment of avulsion fractures of the iliac crest apophysis in adolescents. Injury, 2014. 45(4): p. 721-4.
- Max Pöschl, L.D., Juvenile Osteo-Chondro-Nekrosen 13 March 2013 ed. Handbuch der medizinischen Radiologie Encyclopedia of Medical Radiology 2012: Springer Berlin, Heidelberg. XX, 824
- Caine, D.J., Growth Plate Injury and Bone Growth: An Update. Pediatr Exerc Sci, 1990. 2(3): p. 209-229.
- Porr, J., C. Lucaciu, and S. Birkett, Avulsion fractures of the pelvis – a qualitative systematic review of the literature. J Can Chiropr Assoc, 2011. 55(4): p. 247-55.
- Sanders, T.G. and M.B. Zlatkin, Avulsion injuries of the pelvis. Semin Musculoskelet Radiol, 2008. 12(1): p. 42-53.
- Dompier, T.P., et al., Time-loss and non-time-loss injuries in youth football players. J Athl Train, 2007. 42(3): p. 395-402.
- Faude, O., R. Rößler, and A. Junge, Football injuries in children and adolescent players: are there clues for prevention?Sports Med, 2013. 43(9): p. 819-37.
Autoren

ist Facharzt für Orthopädie und Unfallchirurgie sowie Sportphysiotherapeut. Er ist an der Charité – Universitätsmedizin Berlin, Abteilung Sportmedizin, tätig. Außerdem ist Dr. Kim Teamarzt des Deutschen Fußball Bundes (DFB), Junioren.
Foto Copyright: Thomas Böcker / DFB

ist Facharzt für Chirurgie. Er ist Geschäftsführender Direktor Centrum für Muskuloskelettale Chirurgie (CMSC) an der Charité Universitätsmedizin Berlin. Er ist aktuell 2. Vizepräsident der DGOU und 2. Vizepräsident der DGU. 2025 tritt er die DGU-Präsidentschaft an.
Foto Copyright: W.Peitz / Charité

